Introduction
Asthma is one of the most common diseases of childhood, accounting for almost 800,000 emergency department (ED) visits per year and a quarter of pediatric hospitalizations.1 For severe exacerbations presenting to an ED, 2024 Global Initiative for Asthma (GINA) Guidelines and 2007 National Asthma Education and Prevention Program (NAEPP) Guidelines recommend initial treatment with a short-acting beta2-agonist (SABA), such as albuterol, along with ipratropium bromide and oral or intravenous (IV) corticosteroids.2,3 The 2007 NAEPP Guidelines state that “continuous administration of a SABA may be more effective in more severely obstructed patients,” but no specific recommendations exist regarding the use of intermittent versus continuous albuterol administration.3 Additionally, there are no guideline recommendations for the ideal timeframe to initiate albuterol for a patient in an asthma exacerbation, but the consensus is that delaying albuterol can worsen patient outcomes. While the use of continuous albuterol has historically been limited to use in the pediatric intensive care unit (PICU), increased use in the ED and other non-intensive care unit (ICU) units has shown improvement in clinical and operational outcomes, including treatment success, hospital length of stay (LOS), and time required for respiratory therapists (RTs) to deliver therapy.4–6
The use of automated dispensing cabinets (ADCs) for medication storage and dispensing in hospitals has rapidly increased since the 1990s; over 80% of hospitals reported using ADCs in 2008.7 Within the ED, ADCs can make emergent pharmaceuticals available for critically ill patients. Outside of asthma management, multiple studies document an operational benefit in EDs when stocking medications in an ADC. These benefits include decreased time to medication administration, decreased time spent by pharmacists verifying orders, and improvement in operational efficiency.8–11
In response to a national shortage of concentrated albuterol 2023, our institution standardized all continuous albuterol doses for patients aged 2 years and older with a moderate or severe asthma exacerbation to start at 10 mg/hr rather than a weight-based dose of 0.5 mg/kg/hr (initial max 15 mg/hr). Before this shortage and dose standardization, the hospital’s main pharmacy prepared all continuous albuterol doses upon receipt of an order or dose request. As a result of dose standardization to conserve supply by limiting the higher initial doses of continuous albuterol, continuous albuterol syringes for 10 mg/hr dosing were able to be batched and stocked in the pediatric ED ADC. This study aimed to evaluate operational and clinical outcomes of stocking continuous albuterol syringes for 10 mg/hr dosing in the ED ADC. The authors hypothesize that stocking in the ADC will decrease time to initiation from pharmacist verification, which could lead to improved clinical outcomes by starting therapy faster.
Materials and Methods
Patient Population. This study was a retrospective chart review that occurred at a single institution’s ED. This hospital’s ED is a stand-alone quaternary Level 1 Trauma Center providing acute care to over 50,000 pediatric patients annually. Patients were identified through a search of the electronic medical record (EMR) looking for continuous albuterol orders in the ED between January 1, 2023, and May 31, 2024. The pre-implementation group included encounters from January 1, 2023, to August 31, 2023, and the post-implementation group included encounters from October 1, 2023, to May 31, 2024. There was a washout period during September 2023 that was not included as providers were adjusting to the new practice.
Patients were included if they were 2-17 years old, weighed ≥ 15 kg, presented with a functional diagnosis of asthma, and received continuous albuterol at a dose of 10 mg/hr in the ED. A functional diagnosis of asthma was defined as receiving 3 sequential doses of ipratropium-albuterol nebulized doses and corticosteroids, per our institution’s asthma treatment algorithm consistent with national guidelines.2 Patients were excluded if they had a past medical history of cardiac disease, chronic respiratory disease (including, but not limited to, cystic fibrosis, tracheostomy, and primary ciliary dysfunction), received continuous albuterol at an outside hospital before admission, had a Pediatric Asthma Score (PAS) < 8, no documented baseline PAS, or were initiated on 15 mg/hr of continuous albuterol. Logistical issues related to stocking continuous albuterol syringes in the ADC were also collected in the post-implementation group. Data were collected using REDCap12,13 and included baseline demographics, PAS before and during continuous albuterol therapy (triage, baseline, and at hours 1, 2, and 6), dosing and duration of continuous albuterol, concomitant medications, and ED disposition. Triage PAS is defined as PAS upon presentation before the administration of any medications. Baseline PAS is defined as PAS after three sequential doses of ipratropium-albuterol but before initiation of continuous albuterol.
Outcomes. The primary endpoint for this study is the change in time from the final pharmacist order verification to initiation of first dose of continuous albuterol. Secondary endpoints included duration of continuous albuterol, hospital LOS, ED disposition, change in PAS from baseline at hours 1, 2, and 6 after starting continuous albuterol, rates of increase dose of continuous albuterol, and rate of treatment failure. PAS was scored by respiratory therapists per the institution’s protocol and includes evaluation of respiratory rate, oxygen requirements, auscultation, retractions, and dyspnea.14 A score of 5-7 is equivalent to a mild exacerbation, 8-11 is a moderate exacerbation, and 12-15 is a severe exacerbation.
Patients were defined as having treatment failure if any of the following occurred: required aminophylline infusion, terbutaline infusion, ketamine infusion, more than one magnesium bolus, magnesium infusion, or escalation of respiratory support (high-flow nasal cannula, CPAP, BiPAP, mechanical ventilation) or heliox. Of note, a patient could have multiple reasons for treatment failure. Rates of requiring increased dose of continuous albuterol to 15 mg/hr was not classified as a treatment failure as those patients may have required intensified albuterol therapy rather than truly required escalated systemic therapy or respiratory support, similar to classifications in GINA guidelines.2 Included in the data collection was a triage PAS, baseline PAS, and change between baseline PAS and PAS at hour 1 (with a margin of ± 15 minutes), hour 2 (with a margin of ± 30 minutes), and hour 6 (with a margin of ± 1 hour) after initiation of continuous albuterol. Not every encounter had documented PAS scores for all the previously defined parameters but it was required to have at least a baseline PAS for inclusion. Operational outcomes related to the number of doses utilized from the ADC and waste were also reported for the last month of the post-implementation group, as stocking and refill practices were adjusted throughout the study time period to limit waste but minimize the number of times an ADC was completely stocked out.
Continuous Albuterol Compounding and Storage. All continuous albuterol doses were prepared in the inpatient pharmacy’s sterile compounding room by diluting concentrated albuterol (5 mg/mL) with 0.9% sodium chloride to a total volume of 48 mL, which is then run via programmable pump at 12 mL/hr via nebulization. In the pre-implementation group, as dose requests or new start orders were received, they were then processed by a pharmacist or pharmacy technician and were subsequently prepared and delivered to the bedside. In the post-implementation group, continuous albuterol doses for 10 mg/hr were prepared in advance in batches stocked in the ADC in the ED and restocked based on expiration and depletion rate information provided by ADC. Two studies assessing the stability of albuterol for nebulization determined that a 7-day beyond-use date (BUD) under refrigeration is appropriate.15,16 At this institution, however, the BUD was limited to 4 days under refrigeration as this product was dispensed in Aerogen® syringes (Galway Business Park, Ireland).17 Doses are prepared in sufficient quantity to last four hours per syringe and in the pre-implementation group, the nurse or RT had to request a new dose every four hours.
Statistical Analysis. This study was powered to detect a difference of 20 minutes in the time from pharmacist verification to continuous albuterol initiation pre- and post-implementation. Eighty patients (40 patients in each group) were estimated to detect the above difference with power of 80% at a two-sided significance level of 0.05 using a two-independent sample T-Test. Descriptive statistics were used to analyze the characteristics of each group of our study (pre- and post-implementation). Normally distributed continuous data was evaluated using a Student’s T-Test. Non-parametric continuous data was analyzed using a Mann-Whitney U Test. Lastly, categorical data was evaluated using a Chi-Square Test or Fischer’s Exact Test. Nominal p values are reported. All statistical tests were run on SAS version 9.4 (SAS Institute, Cary, NC).
Results
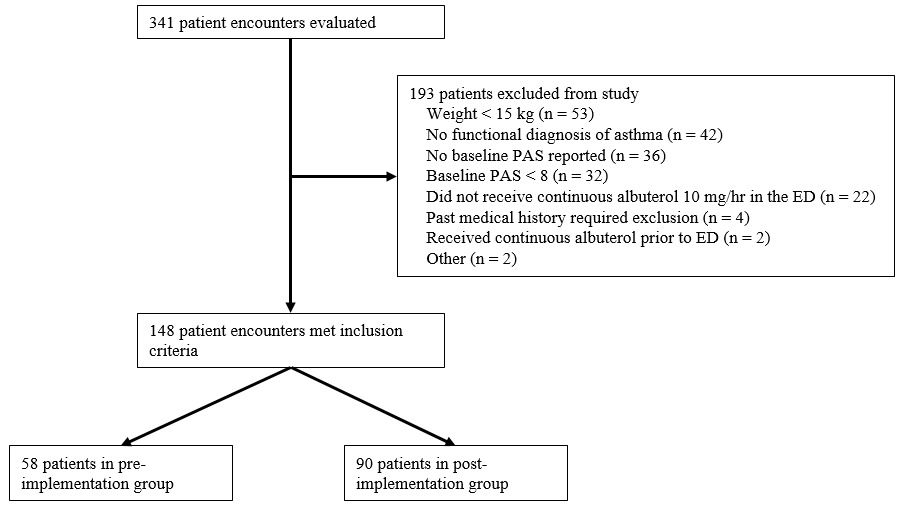
Three hundred and forty-one patients were evaluated for inclusion. One hundred and forty-eight patients were included in the study: 58 in the pre-implementation group and 90 in the post-implementation group (Figure 1). Baseline demographics were well balanced between the two groups, except that the pre-implementation group had a higher rate of Hispanic/Latino ethnicity (20.7% vs 8.9%, p=0.04) (Table 1). Notably, there was no difference in triage or baseline PAS which was used as the marker of clinical severity (Table 1).

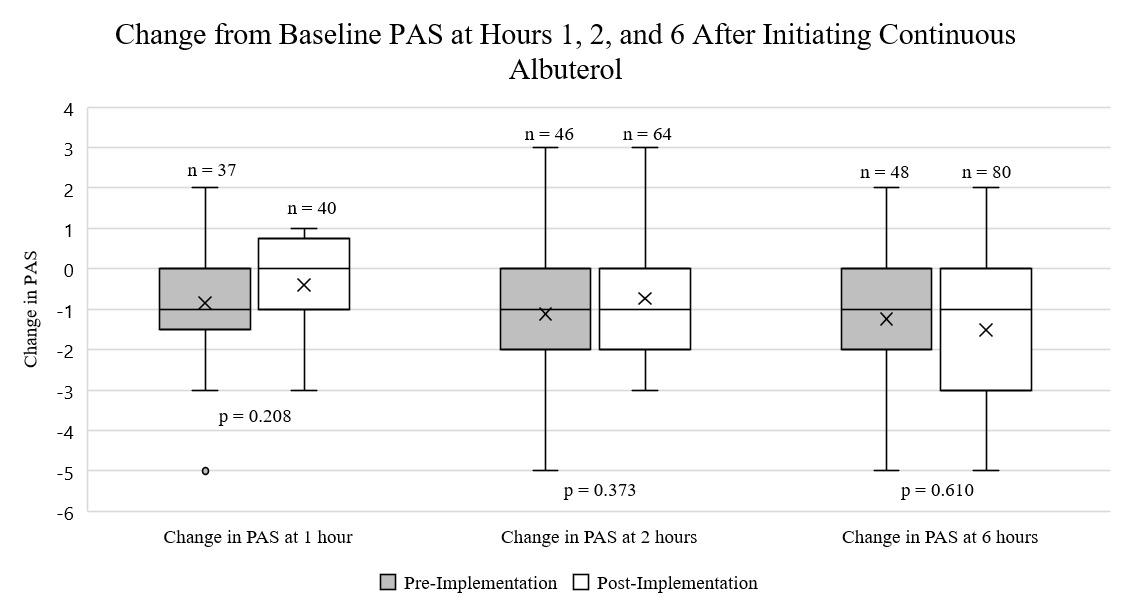
For the primary outcome, the post-implementation group had a decreased time to initiation of first dose of continuous albuterol from verification (47.3 vs 14.7 minutes, p<0.001) (Table 2). A similar decrease was seen in time between the initiation of first dose and ordering by a provider, but no change was found for time required for pharmacist verification (Table 2). Additionally, no changes were seen between hospital LOS, duration of continuous albuterol, ED disposition, or rates of treatment failure (Table 2). The most common reason for treatment failure was receiving more than one magnesium bolus (Table 2). There were no differences in reason for treatment failure between the two groups. Of those who failed, there was no difference in the time to treatment failure (11.5 vs 10.9 hours, p=0.822). There were no differences between groups in change in PAS from baseline PAS at any of the time points (Figure 2). No issues were documented with stocking the continuous albuterol syringes in the ED ADC in the post-implementation group.

In the last month of the post-implementation period (May 2024), 72 syringes were loaded into the ED ADC in batches of a median (IQR) of 6 (4-6) syringes every 48 (31-63) hours. During that month, the maximum PAR was 8 syringes and the minimum PAR to trigger an ADC refill was 2 syringes. An ADC was completely stocked out 4 times versus reaching prompted a replenishment due to reaching the minimum PAR 9 times. Throughout May 2024, 52 syringes were utilized for a patient dose (either the initial or subsequent every 4-hour dose), an average of 1.7 syringes/day.
Discussion
To our knowledge, this study is the first to evaluate the operational and clinical benefits of stocking continuous albuterol syringes for 10 mg/hr dosing in the ED ADC at a pediatric institution. Results showed that batching and stocking these doses in the ED ADC decreased the time between pharmacist verification and initiation of first dose by more than thirty minutes (69% decrease in time to first dose). This decrease in time to initiation aligns with the author’s hypothesis, as proactively stocking in the ADC removes the time required to prepare medication in the main pharmacy IV room and deliver it to the patient and allows for improved workflow for nurses and RTs.
These results align with the current literature. Ward et al8 found that stocking IV vancomycin batched doses in an ED ADC led to a higher proportion of patients receiving vancomycin within 60 minutes of ordering (0% vs 14.7%, p=0.04) without any adverse effects related to dosing appropriateness. This aligns with our study that similarly looked at a single medication being stocked in the ED ADC and found a decreased time to first dose initiation. Portelli et al18 reported the impact of stocking-controlled medications in an in a surgical unit ADC within a hospital. They found a reduction in the number of medication and patient-related errors in the post-ADC group (0.4% vs 0%) and a reduction in the number of hours that pharmacists had to respond to medication requests and inspection of ward stock (9 vs 1 hour per month). A 2024 review article by Borrelli et al9 that included 9 studies evaluating the use of ADCs in perioperative and surgical settings found the implementation of ADCs and stocking medications in this setting decreased medication errors, reduced controlled-substance discrepancies, improved inventory management, and enhanced user experience. While not all these outcomes were able to be evaluated based on data readily available in the EMR for this study, they show the additional benefits that can be anticipated with stocking medications in an ADC.
No changes were seen in any secondary outcomes, including hospital LOS, ED disposition, continuous albuterol duration, PAS at different time points after initiation, and rates of treatment failure. While the patients had well-balanced demographics, including no differences in their severity markers of initial and baseline PAS, the hospital LOS and duration of continuous albuterol did trend towards longer in the post-implementation group without being statistically significant. These trends may be due to confounding factors such as the severity of respiratory season or general hospital census not accounted for in these results.
Stocking practices of the continuous albuterol syringes were variable throughout the post-implementation study period to balance reducing the number of syringes that were outdated and subsequently wasted against an ADC completely stocking out before a refill was able to be processed. While the exact number of syringes that were specifically outdated from that ED ADC is unavailable, it can be assumed that around 25% of doses that were stocked were outdated and potentially wasted, as only 52 of the 72 doses were dispensed to a patient. An institution should carefully consider the usage trends to limit waste on a month-by-month basis, as the use of continuous albuterol is subject to the seasonal changes in respiratory illnesses. In response to this high rate of waste, this institution modified the standard maximum and minimum PAR to be higher during months with peak respiratory illness visits to the ED and lower in all other months. This practice aligned with our institution’s goals during the albuterol shortage, as starting all patients on 10 mg/hr would decrease the number of 15 mg/hr that were initiated on a patient who might have been sufficient on 10 mg/hr, and also allowing batching of the resources to reduce wasting partial vials.
Limitations. This study does have multiple limitations. First, this study was retrospective across two different timeframes which may have had inherent differences that could confound the results. Examples include severity of respiratory season and general hospital census and acuity, as that may have confounded the patient’s length of stay and duration of albuterol. Not all data was able to be collected if it was not documented promptly in the EMR. Second, additional operational impacts were not able to be captured from the institution’s current EMR, including medication error rates for continuous albuterol, changes in pharmacist or pharmacy technician time spent on providing doses, medication requests for continuous albuterol doses, medication costs, and nursing or RT time spent on care for patients. Next, the impact of the operational benefits is unknown at institutions with pediatric institutions with smaller patient volumes or adult institutions with fewer pediatric patients, as the delay may have theoretically be greater to receive first dose of continuous albuterol or optimal stocking practices may vary. Finally, this study only included a single pediatric institution’s emergency department, which may have decreased the external validity of this study at other institutions and may not be generalizable. It was only powered to find a difference in the time to initiation of the first dose of albuterol and was not powered to find a difference in PAS after initiation.
Conclusion
Proactively stocking continuous albuterol syringes for 10 mg/hr doses in a pediatric ED ADC reduced the time from pharmacist verification to dose initiation by almost 70%. There were no changes to other operational or clinical outcomes, including hospital LOS, duration of continuous albuterol, ED disposition, PAS at different time points after initiation, or rates or causes of treatment failure. Institutions should frequently assess their individual usage of medication stocked in ADCs to optimize quantity stocked to avoid waste. Further studies are needed to determine the other clinical and operational impacts of stocking continuous albuterol syringes and other emergent medications in an ED ADC.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare no conflicts or financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, gifts, and honoraria. The authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors attest to meeting the four criteria recommended by the ICMJE for authorship of this manuscript.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available because they contain information that could compromise the privacy of research participants.
Author Contributions (CRediT)
Sadie Fugate: Data curation, Validation, Formal analysis, Writing – original draft, Writing – review & editing.
Allison Mack: Data curation, Validation, Formal analysis, Writing – original draft, Writing – review & editing.
Benjamin Nti: Conceptualization, Methodology, Validation, Formal analysis, Writing – review & editing.
Matthew Hays: Formal analysis, Writing – review & editing.
Xiaochun Li: Formal analysis, Writing – review & editing.
Allison M. Kenneally: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing.