Introduction
The Centers for Disease Control and Prevention (CDC) estimated 139.8 million visits to emergency departments (ED) in 2021.1 Evaluation for suspected bacterial infection is common, and associated microbiological results often finalize after ED discharge, requiring reliable post-discharge culture follow-up workflows to ensure timely, accurate action on new information. Effective culture follow-up services aim to rapidly review finalized results and promptly contact patients when an intervention is needed. Interventions might include optimizing or discontinuing antibiotics, communicating results to primary care, arranging additional testing, and providing patient education.2 By facilitating appropriate antimicrobial therapy, these programs help reduce treatment failure and other downstream harms.
Implementation models vary widely across institutions. Reported personnel include medical doctors (MDs), advanced practice practitioners [APPs, including nurse practitioners (NPs) and physician assistants (PAs)], clinical pharmacists and pharmacy residents, microbiology lab staff, and registered nurses (RNs) – often in different combinations and with differing scopes of responsibility.2 Although many EDs incorporate clinical pharmacists in culture follow-up review services, direct, contemporaneous comparisons of programs with versus without pharmacist involvement remain limited. This study compares the time from culture result to initial review between a main ED with clinical pharmacist involvement and two external EDs without pharmacist involvement. Secondary outcomes evaluate process and safety domains, including time to first attempted patient contact and errors in callback interventions.
METHODS
Study Design and Setting
This single-center retrospective, observational, cohort study was approved by the East Alabama Health (EAH) and Auburn University Institutional Review Boards with waived informed consent. Guidance from the EQUATOR Network was utilized in the development of this study and manuscript.3,4 The study site, East Alabama Health, serves an 11-county area and is comprised of a main hospital and ED, a free-standing ED (FED), and a rural emergency hospital (REH). The main hospital ED has 34 beds serving around 40,000 patients per year, the FED has 12 beds serving around 25,000 patients per year, and the REH has 10 beds serving around 16,000 patients per year.
Culture Follow-Up Workflow
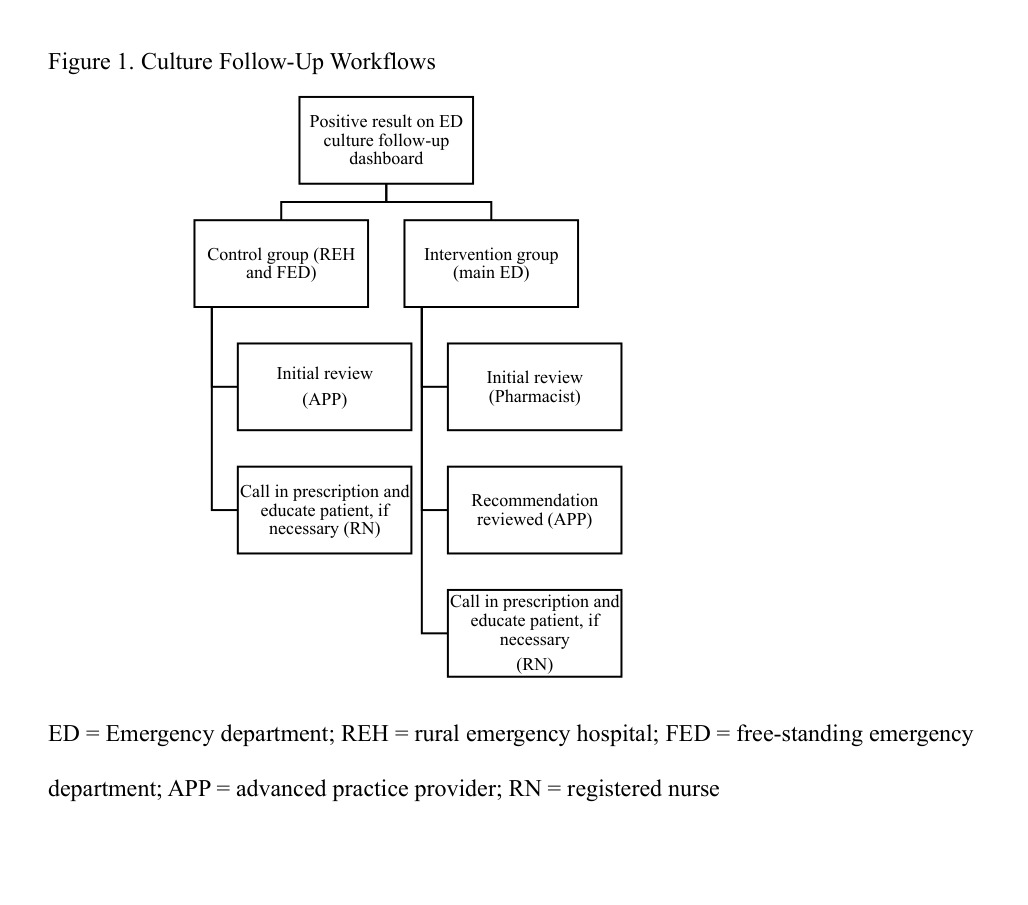
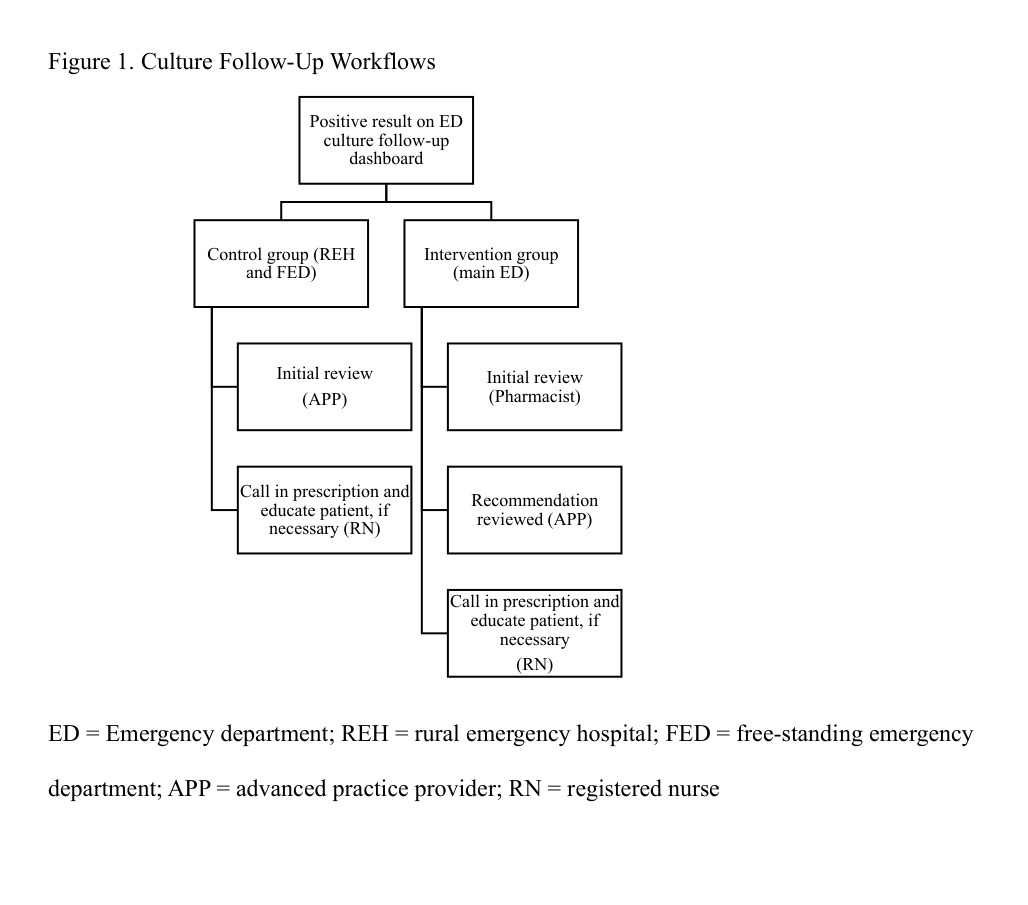
Within the main ED, pharmacists initially perform culture review with final review by an APP. As with the APPs, this task is in addition to their normal workload. For the FED and REH, APPs are responsible for culture review without pharmacist involvement. Review and assessment take place during the shift and vary based on location. Pharmacists cover daily at the main ED from 11:00 a.m. to 10:00 p.m. while APPs cover 24h at the FED, and 12h at the REH. At each location, microbiological culture results populate on an ED culture follow-up dashboard within the electronic health record (EHR), Cerner™. In real-time, the dashboard populates positive results that finalize post-discharge from the ED and also links to the patient’s profile and relevant ED visit within the EHR. Personnel can write comments and free-text recommendations within the ED culture follow-up dashboard. Within the main ED, pharmacists provide free-text recommendations within the ED culture follow-up dashboard and flag the item for provider review. The provider either accepts, rejects, or modifies the recommendation and a registered nurse calls in the prescription to the patient’s preferred pharmacy. The registered nurse attempts to call the patient, leaves voicemails as necessary, and sends a letter if no call back received. A callback qualifies for completion if the following conditions are met: (1) patient is contacted, or (2) if a message is left by the nurse. If no answer, the nurse makes a second attempt in 24 hours. If no answer after the second call, a letter is sent to the patient. Of note, positive blood culture results are phoned to the charge RN before populating on the ED culture-follow-up dashboard. Workflow for the intervention and control group is described in Figure 1.
Study Population
The study evaluated patients who had positive microbiology data resulting after discharge from any of the three EDs between August 2023 through February 2024. Patients were excluded from the study if they were discharged to comfort care or hospice from the ED, were admitted to EAH as inpatient from the ED, were transferred to another facility from the ED, or if they expired during their ED visit.
Data Collection
The institution’s EHR was utilized to generate a list of patients from all three EDs with cultures resulting post-discharge. Data were collected from chart review by two study team members, with complex cases brought to the primary author for adjudication. Authors decided a priori to include 300 patients in the study with 150 patients from the main ED and 75 patients from each external ED as a convenience sample to ensure project completion during the pharmacy residency year. Based on an estimated reduction in time to initial patient contact of approximately 12 hours per prior literature, 256 patients would be needed to meet 80% power with alpha set at 0.05. This power calculation supported our convenience sample of 300 patients.5–10
Outcomes
The primary outcome was time from culture result to initial culture review. Culture result time was defined as the time the culture was marked as finalized by the microbiology laboratory. Secondary outcomes included time from culture result to first attempted patient contact. Time of first attempted patient contact was defined as the first time documented within the health record (within the ED culture follow-up dashboard) that personnel attempted to contact the patient. Other secondary outcomes included type of pharmacist intervention (e.g. agent changed, dose changed, duration changed); acceptance rate of pharmacist interventions by APP; method and necessity to contact patient; and accuracy of callback interventions. Definitions of potential callback intervention errors were determined a priori through consensus among study investigators. The primary author (a PGY-2 emergency medicine pharmacy resident at the time of data collection) assessed for errors, with adjudication by the senior author, a board-certified infectious disease pharmacist). Errors were categorized as follows: antimicrobial not active against the identified pathogen (“bug-drug mismatch”); incorrect antimicrobial dose/frequency (based on the institution’s pharmacy and therapeutics committee-approved renal dosing protocol, supplemented with UpToDate® Lexidrug™ for agents not included in the protocol); duration shorter than guideline recommendations; allergy to prescribed antimicrobial; no documentation of patient contact or follow-up by callback nurse; antimicrobial initiation with no indication (e.g., asymptomatic bacteriuria treatment); no review performed by APP or pharmacist; and prescription that differed from the intended order as documented in the culture follow-up dashboard.
Consistent with Clinical & Laboratory Standards Institute (CLSI) guidance, intravenous cefazolin breakpoints were used to predict susceptibility for oral cephalosporins commonly used for uncomplicated urinary tract infections, and ampicillin susceptibility was used to infer activity of amoxicillin.11
We also assessed rate of prescriptions filled after culture follow-up contact, using insurance claims data in the external fill history from the EHR; rate of hospitalization for the same condition within thirty days; and rate of ED re-visit.
Statistical Analysis
Data analysis was conducted via IBM SPSS version 30.0.0.0. Categorical data was analyzed via Pearson’s chi-square or Fisher’s exact test and are reported as n (%). Continuous data was analyzed via Student’s t-test or Mann-Whitney U based upon distribution and reported as mean ± SD or median [IQR] respectively. Statistical significance was defined by a 2-tailed p-value < 0.05.
RESULTS
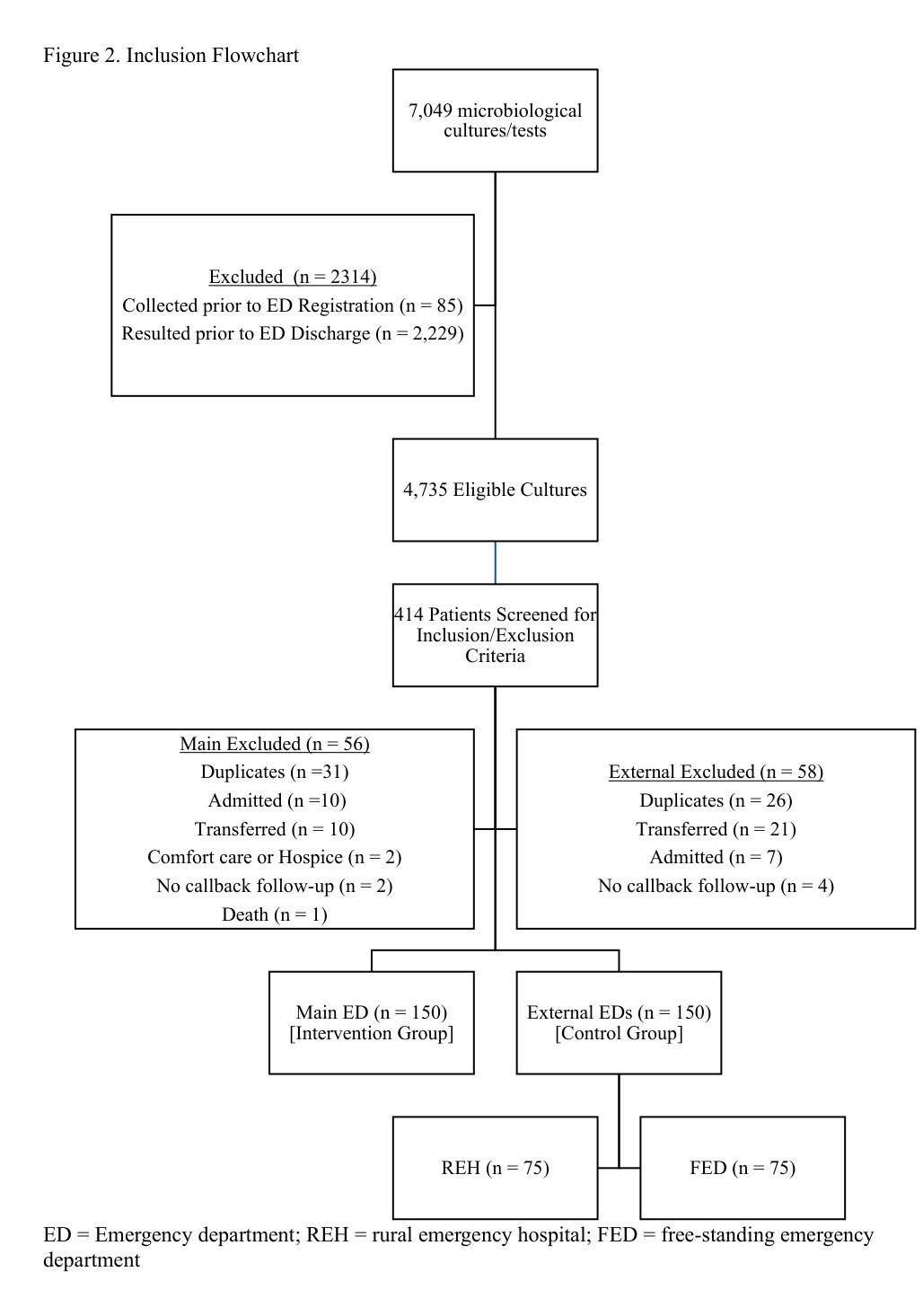
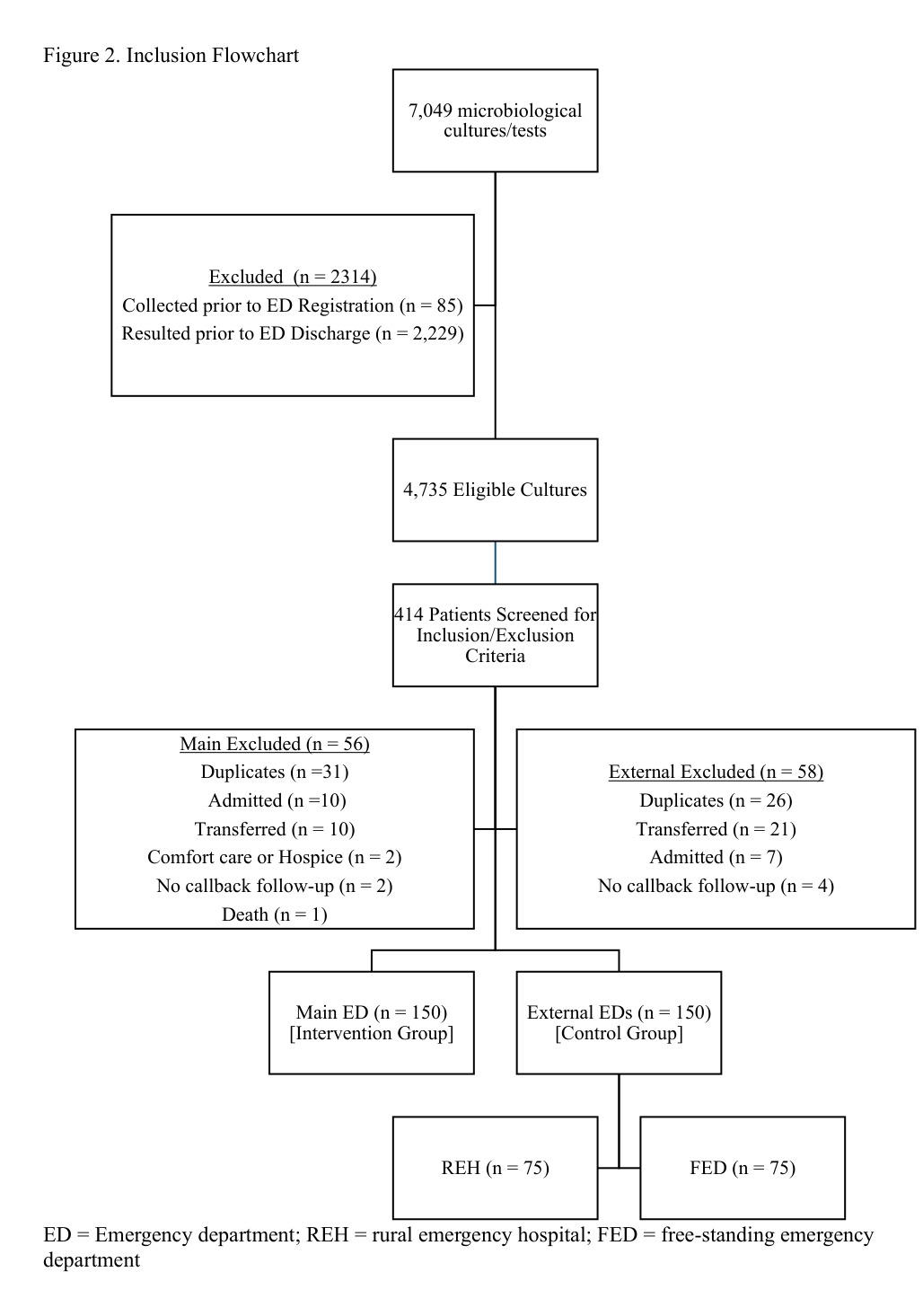
A total of 7,049 microbiological cultures were screened during the study period. Of these, 2,314 were excluded (85 collected prior to registration in the ED; 2,229 resulted prior to ED discharge), leaving 4,735 eligible cultures. From these, the patient list was randomized to minimize temporal bias, and patients were reviewed until the target of 300 patients was met. In all, 414 patients were reviewed for inclusion/exclusion criteria until the target of 300 patients was met; 114 patients were excluded (main ED, n=56; external EDs, n=58), most commonly for duplicate encounters (Figure 2). The final cohort included 300 patients (main ED, n=150; external EDs, n=150).
Baseline characteristics are shown in Table 1. Patients in the main ED were older (median age 52 years [IQR 27-74] vs. 39.5 years [IQR 23-66.3]; p = 0.016) and were less likely to present to the ED for infection (64.0% vs. 76.7%; p = 0.023). The distribution of culture types was similar between groups, with urine cultures predominating (main ED 76.0% vs. external 72.0%), followed by pustule/abscess cultures (10.0% vs. 9.3%).
The median time from culture result to initial review was significantly shorter at the main ED with clinical pharmacist involvement (median 3.1 hours [IQR 1.1-5.3]) than at the external EDs without pharmacist involvement (median 8.8 hours [IQR 3.8-23.9]; p < 0.001). Time from result to callback completion was also shorter in the intervention group (5.2 hours [IQR 1.7-27.3] vs. 25.0 hours [5.8-57.6]; p < 0.001). Initial review was performed by pharmacists in 88.7% of main ED encounters and by APPs in 96.7% of external ED encounters (p<0.001). Median time from culture result to time that a new prescription was sent/called in did not differ, nor did the time from culture result to first attempted patient contact (Table 2).
Errors in ED callback interventions were less frequent in the main ED with pharmacist involvement (error-free callbacks 96% vs. 81%, p = 0.001). In the control group, the most common error type was antimicrobial initiation without indication: 10 of 11 cases involved inappropriate treatment of asymptomatic bacteriuria (ASB), and one case involved antibiotic treatment for diarrhea. Two patients in the control group received antibiotics despite documented allergies (one sulfonamide allergy prescribed trimethoprim/sulfamethoxazole; one penicillin allergy prescribed amoxicillin/clavulanate). Five errors reflected untreated infectious indications in the control group (bacteremia, Gardnerella vaginalis, CTDNA-positive, and two wound/tissue infections). Notably, the bacteremia case had been documented by an APP as “no action needed” and was later identified by a stewardship pharmacist upon review of blood culture reports, leading to the patient returning to the ED for treatment. Within the main ED, one untreated indication error occurred when a patient with pyelonephritis was treated with nitrofurantoin. In this case, despite being in the pharmacist-integrated model, the culture was not reviewed by a pharmacist. Of the 6 total errors in the main ED group, only two were attributable to pharmacist actions: one instance of ASB treatment following pharmacist recommendation and one dosing error in which amoxicillin was prescribed TID rather than renally adjusted BID for reduced renal function. All remaining errors originated from downstream RN or APP actions rather than pharmacist review.
There were no statistically significant differences between groups in the rate of prescription fill after contact, 30-day hospitalization for the same condition, or ED revisit. Detailed outcomes appear in Table 2.
DISCUSSION
In this contemporaneous, multi-ED comparison, integrating clinical pharmacists into ED culture follow-up was associated with substantially faster initial review and patient contact and with fewer errors in callback interventions. The absolute median improvement in time to review was ~5 hours, and the pharmacist-integrated model achieved callback completion nearly five times faster, underscoring a meaningful operational and safety advantage in acting on finalized microbiology. Timelier review and outreach can prevent treatment delays for resistant or mis-targeted infections, reduce unnecessary antimicrobial exposure when cultures indicate no treatment is warranted, and accelerate communication of results and follow-up plans – all patient-safety benefits in the post-discharge window. Our findings align with the overall direction of prior work demonstrating that pharmacist-involved programs shorten time-based outcomes and improve process reliability in ED culture follow-up models.
In this study, time from culture result to initial review was reduced in a main ED with pharmacy involvement. This aligns with other studies evaluating clinical pharmacist integration in culture follow-up, which consistently demonstrate time benefits with pharmacist involvement.5–9,11 In previous literature, time from culture result to initial review among ED culture follow-up programs ranged from 0.8 to 47.9 hours.2 The median time in our study of 3.1 hours was within this range and on the faster end of this range. This might be explained in part by the real-time dashboard integrated within the EHR for culture follow-up results and documentation of actions. Published studies use heterogeneous time endpoints—e.g., time from result to review, time to patient notification/contact, and time to order entry or therapy optimization—and differ in staffing models (dedicated pharmacist hours vs pharmacists embedded in broader clinical duties), hours of coverage, and division of labor between pharmacists, APPs, and RNs.5–20 Against this backdrop, the absolute median reduction of ~5 hours in time to initial review observed here is directionally consistent with pharmacist-integrated programs and sits within the range reported by before–after and service-implementation studies. It is important to note that our study observed a reduction in time to initial review, even though pharmacists were not dedicated to culture review exclusively. This context supports the external validity of our work while acknowledging that endpoint definitions and operational designs drive between-study variability.
Our study also saw a significant reduction in callback-intervention errors with pharmacist oversight, which is clinically and operationally important. Notably, while all errors represent opportunities for process improvement, a subset of errors were potential harmful clinically. No harmful errors occurred in the pharmacist-integrated model, whereas 14 occurred in the external EDs. These included untreated infections, dosing errors, antimicrobial prescribing in the setting of documented allergy, and cases in which the final dispensed prescription did not match the intended order. The disproportionate number of harmful errors in the external EDs reinforces the value of pharmacist adjudication, particularly during complex decision-making scenarios.
Several errors (e.g., inappropriate treatment of asymptomatic bacteriuria) were unlikely to cause short-term harm but nevertheless reflect modifiable stewardship opportunities. In the external EDs, the leading error was initiating antimicrobials without indication (7%), with 10 of 11 cases due to inappropriate treatment of ASB. Almulhim and colleagues found a higher percentage of appropriate interventions in the pharmacist group compared to an APP group, also driven largely by the inappropriate treatment of ASB.21 These patterns suggest complementary improvement opportunities: (1) targeted stewardship education and (2) culture ordering guidance (e.g., limiting urine cultures when symptoms are absent) to prevent cascades that drive unnecessary treatment.
Despite earlier review and outreach, the time from result to first attempted patient contact and to new prescription sent was similar between groups. This step was largely RN-driven after provider sign-off in both models, creating a common downstream bottleneck that attenuates any upstream gains from faster pharmacist review. In some ED culture follow-up models, clinical pharmacists assume responsibility for the full continuum of after-visit result management, including entering and pending antimicrobial orders directly, requiring only an APP co-signature, and completing the patient callback themselves.10,22 Such models reduce reliance on downstream RN-driven communication steps and may mitigate transcription errors that arise when free-text recommendations must be manually relayed. Still other culture follow-up models include collaborative practice agreements in which pharmacists can independently prescribe and make medication changes.18,23 Jurisdictional variability in collaborative practice agreement requirements may influence the feasibility of fully pharmacist-led pathways; however, these examples illustrate that expanding pharmacist authority can streamline the entire culture follow-up process and potentially amplify timeliness gains.
As in several prior reports, our study did not detect differences in 30-day hospitalization or ED revisits.6,7,10–12,18,24–26 Given the sample size and the multifactorial nature of these endpoints, the study may be underpowered to detect modest differences; moreover, social and access factors (transportation, pharmacy hours, out-of-pocket costs) likely dilute the effect of process improvements on utilization metrics. These null findings should not be interpreted as lack of clinical value; rather, they highlight the need for larger, possibly multicenter evaluations and for patient-centered outcomes (symptom resolution, adverse drug events, satisfaction) that are more proximal to stewardship impact.
Strengths and Limitations
Strengths include the contemporaneous, head-to-head comparison of pharmacist-integrated versus non-pharmacist models within the same health system and standardized use of an ED culture follow-up dashboard, as well as inclusion of diverse culture types. External generalizability is strengthened by the fact that clinical pharmacy involvement in culture follow-up services were not available 24 hours a day within the intervention group. Key limitations include baseline imbalances (age, presenting complaint), single-center design, reliance on EHR timestamp proxies (with potential overestimation of blood-culture timeliness because critical results are phoned to the charge RN before final result time), and use of claims-based fill history that may undercount cash prescriptions. Additionally, two cases in the control group were reviewed by a pharmacist. APPs at external EDs could informally consult pharmacists, potentially biasing effects toward the null, though there was no formalized process or assigned duties for pharmacists to review culture follow-ups at external EDs. Finally, the study was not powered for clinical utilization outcomes.
CONCLUSION
Our results support integrating clinical pharmacists into ED culture follow-up as a pragmatic means to accelerate action and reduce errors. Further, the reduction in errors may be used as support for development of collaborative practice agreements or pharmacist prescribing in jurisdictions where pharmacists are eligible for advance practitioner privileges. Future research should evaluate cost-effectiveness, patient-reported outcomes, time from order to medication in hand, and coverage models (e.g., after-hours or 7-day service). Workflow downstream from initial review should be evaluated to improve timeliness of patient contact. Studies should also compare pharmacist-led models with enhanced APP training to determine whether similar gains in timeliness and error reduction can be achieved.
Ethical considerations
This study received ethical approval from the EAMC and Auburn University IRB (approval #24-12-E) on August 22, 2024. This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Consent to participate
This study received ethical approval from the EAMC IRB (approval #24-12-E) on August 22, 2024 and Auburn University IRB (approval #STUDY00000016) on September 16, 2024.
Consent for publication
Not applicable
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding statement
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
Patient data will not be shared with third parties.
Acknowledgments
No acknowledgments were reported in the supplied materials.
Author Contributions (CRediT)
Conceptualization: EWC; Data curation: EWC, LJC, NCP; Formal Analysis: EWC, LJC; Funding acquisition: ; Investigation: EWC, LJC, NCP, JED; Methodology: EWC, JED; Project administration: EWC; Resources: EWC; Software: EWC; Supervision: EWC; Validation: EWC; Visualization: EWC; Writing – original draft: EWC, LJC; Writing – review & editing: EWC, LJC, NCP, JED