Introduction
Nicardipine is an intravenous dihydropyridine calcium channel blocker indicated for short-term management of hypertension in the inpatient setting. It is available as premix bags at concentrations of 0.1 mg/mL and 0.2 mg/mL.1 Additionally, a 2.5 mg/mL vial is available with manufacturer recommendations to dilute to a final concentration of 0.1 mg/mL.
In efforts to standardize medication concentrations and reduce errors, the American Society of Health-System Pharmacists (ASHP) maintains infusion standards for adult and pediatric continuous infusions. These standards endorse concentrations of 0.1, 0.2, and 0.5 mg/mL in pediatric patients, but limit concentrations to only 0.1 and 0.2 mg/mL in adult patients.2,3 This may be attributed to the lack of data establishing the safety of high-concentration nicardipine in adult patients. Even in the pediatric population, available literature is scarce and limited to three small case reports including 3 to 29 patients with nicardipine concentrations ranging from 0.5 to 3.6 mg/mL.4–6
Despite the availability of small case reports in pediatric patients, safety data for high-concentration nicardipine in adults remain a crucial gap in literature. The administration of high-concentration nicardipine presents advantages such as minimized volume load and reduced therapeutic cost. Demonstrating its safety could have important implications for the management of hypertensive emergencies and severe hypertension. The primary objective of this study was to evaluate the safety of high-concentration nicardipine, defined as a concentration of 0.5 mg/mL, in adult patients.
Methods
This was a retrospective, observational, single-center study completed at a 576-bed academic medical center. This institution utilizes a standard nicardipine concentration of 25 mg/110 mL (0.23 mg/mL) normal saline with an alternative high-concentration formulation of 50 mg/100 mL (0.5 mg/mL) available for patients requiring fluid restriction. Institutional standards advise for central line administration for high-concentration nicardipine.
All adult patients receiving high-concentration nicardipine, defined as 0.5 mg/mL, between January 1st, 2014, and September 16th, 2024, were evaluated for inclusion. Those on nicardipine for less than two hours were excluded from the study. Relevant patient information including demographic characteristics (age, weight, height, body mass index, sex, reported race), clinical parameters (hospital length of stay, admission disposition, location at nicardipine initiation), treatment details (ordering service, nicardipine indication), and detailed infusion specifications (concentration, duration, rates, administration sites) were extracted from the Cerner Powerchart electronic medical record system.
Indications for nicardipine were collected retrospectively based on review of blood pressures and provider documentation and defined in accordance with guideline definitions for hypertension (SBP ≥ 130 mmHg and/or DBP ≥ 80 mmHg), severe hypertension (SBP > 180 mmHg and/or DBP > 120 mmHg), and hypertensive emergency (SBP > 180 mmHg and/or DBP > 120 mmHg PLUS evidence of new onset or worsening organ damage).
To identify concentration-related ADEs, a chart review was conducted. This included an analysis of nursing documentation in the ‘Vascular Access Device’ section of the ICU flowsheet for up to 24 hours post-infusion, a review of provider notes, and a chart search using the key terms: erythema, extravasation, infiltration, phlebitis, thrombophlebitis, irritation, infusion site pain, and infusion site reaction. Additionally, an event reporting database from Origami Risk, Incident Reporting Information System (IRIS), was utilized to capture all reported ADEs related to administration of IV nicardipine during the timeframe of interest.
All data collection was recorded and stored in the online RedCAP database with descriptive statistics analyzed using Microsoft Excel software (2018). Data collection was performed by four investigators who received training from the primary investigator and creator of the data collection tool. The collection tool included clarifying remarks, definitions of outcomes, and reminders to ensure consistency across investigators. The finalized dataset was audited by the primary investigator and statistician. This study received institutional review board approval with waiver of patient consent (IRB#PHX-24-500-465-71-47).
Results
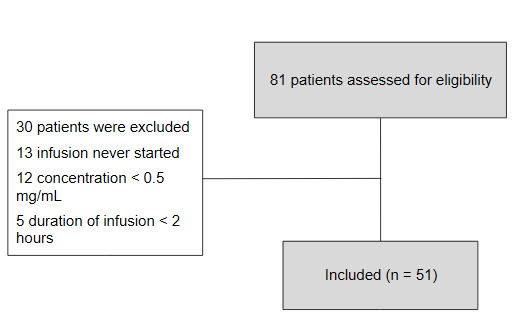
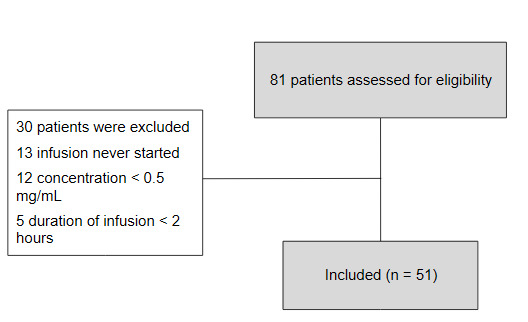
A total of 81 patients were initially identified for inclusion. Thirty of these patients were subsequently excluded for the following reasons: the order was never initiated, the drug preparation was incorrect (concentration < 0.5 mg/mL), or the infusion was discontinued within two hours (Figure 1).
Baseline characteristics are presented in Table 1. The median age was 55 [41-64.5] years old. and 70.6% were male. The median body mass index at admission was 31.9 [27.6-36.6] kg/m2. Nicardipine utilization data are presented in Table 2. Primary indications for nicardipine therapy were hypertension without organ damage (47.1%) and hypertensive emergency with evidence of new onset or worsening end-organ dysfunction (43.1%). Patients were primarily in the ICU (98%) when the infusion was started with the highest utilization by the neuroscience ICU (56.9%). The predominant ordering services were critical care (58.8%) and neurology (29.4%). The median initial infusion duration was 27.4 [10.3-58.9] hours . Most patients (72.5%) received high-concentration nicardipine through central venous access with a notable finding of 17.6% and 9.8% receiving the infusion through a peripheral and midline catheter, respectively. Notably, no ADEs were observed throughout the study population.
Discussion
This retrospective, observational, single-center study is the first to explore the administration of nicardipine at a high concentration of 0.5 mg/mL in adult patients, addressing a significant gap in the available literature. While ASHP includes 0.5 mg/mL nicardipine in its pediatric infusion standards, this concentration is excluded from the adult standards, likely due to a lack of safety data in that population.2,3 Our findings indicate that high-concentration nicardipine was administered safely, with no ADEs reported in the study population. These results echo the safety data previously reported in pediatric studies and have important implications for antihypertensive selection in the acute setting, particularly when considering fluid volume, cost, and clinical efficacy.
Small case reports have previously endorsed safe administration of high-concentration nicardipine, ranging from 0.5-3.6 mg/mL, in pediatric patients with minimal adverse events in those receiving the medication peripherally.4–6 In a case report of three pediatric patients, Michael et al4 reported routinely using concentrations of nicardipine up to 0.5 mg/mL without adverse events outside of occasional superficial thrombophlebitis. A subsequent case report by Tenny et al5 evaluated seven pediatric patients receiving nicardipine at concentrations between 0.9 and 3.6 mg/mL. They observed thrombophlebitis in two patients receiving peripheral administration but noted no complications with central administration. Lastly, in a retrospective study by Flynn et al. of 29 children receiving nicardipine 0.5 mg/mL, only minor ADEs were observed, with tachycardia being the most prominent.6 The authors concluded that the minimal ADEs observed were attributable to its pharmacological properties rather than the concentration used or administration route. Although these studies provided some evidence of safety of high-concentration nicardipine, they contained a small number of pediatric patients and larger studies in an adult population are essential in order to confirm these safety outcomes.
Of note the stability of nicardipine 0.5 mg/mL has been demonstrated in one prior study. Baaske et al tested both nicardipine 0.5 mg/mL and 0.05 mg/mL in eight IV solutions at room temperature under normal fluorescent light and found that while drug concentrations slowly decreased in polyvinyl chloride (PVC) containers starting as early as 24 hours, both concentrations remained stable in the majority of solutions tested with no evidence of degradation for up to seven days.7 The drug was found to be unstable in 5% sodium bicarbonate and PVC bags containing lactated ringers. Of note, our institution compounds high-concentration nicardipine infusions in PVC containers with 0.9% normal saline which maintained its concentration above 95% up to seven days within the study. In accordance with institutional policy and sterile compounding standards, this facility assigns all IV nicardipine compounds a beyond-use date of 24 hours.
Our retrospective chart review and event reporting database did not observe any ADEs, including extravasation, throughout the study population. As IV nicardipine is considered an irritant and not a vesicant, typical extravasation management consists of drug aspiration, cold or warm compress, and limb elevation.8 Unfortunately the above actions were difficult to capture via retrospective chart review. The investigators however were able to assess the utilization of hyaluronidase as an off-label therapy for extravasation and confirmed that none of the patients included in the study received hyaluronidase during their admission. This is in accordance with the lack of ADEs found and further validates the study findings.
The outcomes reported introduce new valuable insights and considerations for intravenous agent selection in the acute setting, particularly when choosing between nicardipine and clevidipine. Clevidipine is generally favored in the setting of hypervolemia as standard concentration nicardipine necessitates greater quantities to achieve clinically similar effects compared to clevidipine. This difference can equate to 25–75 mL/hr of nicardipine 0.2 mg/mL in comparison to 2–64 mL/hr of clevidipine 0.5 mg/mL.1,9 Establishing the safety and availability of a high-concentration formulation would enable providers to reduce the infusion volume of nicardipine to 10–30 mL/hr, making it comparable to clevidipine.
From a financial standpoint, nicardipine presents a significantly more cost-effective option. As of June 2025, a 25 mg/10 mL (2.5 mg/mL) vial of nicardipine costs approximately $8.72 with one to two vials needed for standard or high-concentration preparations, respectively.10 In contrast, a 100 mL vial of clevidipine 0.5 mg/mL costs approximately $157.91. A recent multicenter retrospective study by Johnson et al in 182 critically ill patients highlighted this disparity, noting a 682% higher average wholesale price for clevidipine.11 While the study found clevidipine reduced medication-associated fluid volume compared to nicardipine (222 mL vs. 518 mL, P = 0.01), the total fluid intake between the two groups was comparable (3,370 mL vs. 3,383 mL, P = 0.43). Clinical outcomes were equivalent between the groups, including time to blood pressure goal (P = 0.37).These findings highlight the reason current hypertension guidelines acknowledge the lack of evidence on which first-line antihypertensive agents offer the greatest benefit in hypertensive emergencies and why no specific agent is preferred.12 This emphasizes the value of utilizing high-concentration nicardipine, as it achieves comparable clinical outcomes and manages fluid balance effectively without incurring additional costs.
Strengths of this study include that it is the first to explore high-concentration nicardipine in adult patients, while also including a larger patient population than those in the pediatric literature. The evaluation of infusion-related safety events was robust as investigators assessed a variety of indicators, including infusion site pain/reaction, erythema, extravasation, phlebitis/thrombophlebitis, and irritation. Adverse drug events were also explored in two modalities through chart review and an institutional incident reporting database.
Limitations of this study can be attributed to its retrospective nature, including potential for incomplete or inaccurate documentation, as well as unreported drug-related events. In efforts to address this, two modalities were utilized to identify events, with the chart and reporting database searches expanded to capture as many events as possible. Moreover, although line type was captured, the size or gauge of IV utilized was not collected. Additionally, 12 patients were unexpectedly excluded as a concentration of 50 mg/120 mL (0.42 mg/mL) was made instead of 0.5 mg/mL due to differences in compounding practices. Lastly, while institutional standards recommend administration of high-concentration nicardipine through a central line, 17.6% and 9.8% of patients received the medication peripherally and via midline, respectively. While this deviation from institutional protocol called for education across disciplines, it incidentally revealed the potential for the exploration of safety in non-central line administration in future studies.
Conclusions
The administration of nicardipine at a concentration of 0.5 mg/mL appears to be safe in adult patients, with no ADEs having occurred during the study period. High-concentration nicardipine is a low-volume, cost-effective alternative to standard-concentration nicardipine and other IV dihydropyridine calcium channel blockers. The establishment of its safety in adults can have significant implications for the short-term treatment of hypertension. Future prospective, multi-center studies are warranted to confirm these findings in a larger, more diverse patient population and to formally evaluate the safety of administering this concentration through non-central access routes.
Key Points
-
High concentration intravenous nicardipine at 0.5 mg/mL was safely administered to adult patients in this study, with no observed adverse drug events related to the infusion.
-
This study represents the first exploration of 0.5 mg/mL nicardipine use in a cohort of adult patients, addressing a current gap in the literature and providing valuable safety data.
-
The findings suggest that high-concentration nicardipine can serve as a low-volume, cost-effective alternative for the short-term management of hypertension in adult patients.
Conflict of Interest and Funding Disclosure
The authors have no conflict of interest or funding to disclose.
Data Availability
The data underlying this article will be shared on reasonable request to the corresponding author